Enteral feeding refers to the provision of a nutritionally complete liquid feed via a tube which leads directly into the stomach or small intestine. This feeding process provides all the necessary carbohydrates, proteins, fats, vitamins, minerals and water.
There are a number of methods by which enteral feeding can be provided i.e. via the nose or via a stoma in the abdominal wall (a surgical opening through which the tube is inserted). Specialist advice is required regarding decisions pertaining to the most appropriate method of enteral feeding in each individual case.
A nasogastric tube (NG tube) is inserted via the nose into the stomach. An NG tube is indicated for short term use only, ideally less than 4 weeks. It can be easily removed when no longer required. Staff should be aware that an NG tube can affect the safety of the swallow if the patient is also taking some nutrition orally.
Gastrostomy or jejunostomy tubes are inserted via a stoma in the abdominal wall into the stomach or intestine. This is a surgical procedure. 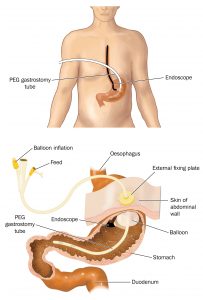
Examples of these tubes are:
- Percutaneous endoscopic gastrostomy tube (PEG tube).
- Radiologically inserted gastrostomy tube (RIG tube).
- Jejunostomy tube inserted into the small
intestine. - Gastrostomy tube with jejunal extension.
Guidance for Maintaining an Enteral Tube In Situ
Following brain injury, the patient with significant cognitive impairment, agitation and/or other behavioural difficulties may not understand why they need to have an enteral feeding tube in place and may try to remove it. Prevention of tube removal is especially important in the first six to eight weeks after initial tube insertion. Gastrostomy or jejunostomy tube removal during this period is likely to damage the stoma and will likely necessitate a further surgical procedure in order to insert a new tube.

When considering enteral feeding and subsequent maintenance of the tube in situ, the patient’s capacity to make informed decisions with regard to such intervention should be assessed by a suitably qualified medical professional. If the patient is assessed as lacking capacity and enteral feeding is deemed necessary, the Adults with Incapacity (Scotland) Act 2000 should be considered in order to legally proceed with the intervention. A Section 47 form will need to be completed by the responsible doctor.

Helpful strategies to prevent tube removal include:
- Regular orientation of the patient to their circumstances if cognitive difficulties are impacting upon tube maintenance.
- Reassurance and explanation about the purpose of the tube.
- Distraction from preoccupation with the tube and redirection of attention to an alternative activity.
- Maintenance of the stoma site to ensure the patient is not experiencing pain or discomfort from an infected stoma site.
- Treatment of stoma infection as necessary.
- Addressing any contributory behavioural (e.g. agitation) or psychiatric difficulties (e.g. anxiety). This may include pharmacological and/or behavioural strategies.
- One-to-one nursing support may need to be considered in some cases.
At times it may be necessary to utilise physical measures to help prevent tube removal. Specialist advice should be sought to ensure that any physical method used would not be considered a form of restraint (follow local protocols). It is important to recognise that these measures may themselves actually increase levels of anxiety, distress and agitation in some patients. Physical measures may include:
- A pouch for a gastrostomy tube which the person may find difficult to open (e.g. G-Tube belt pouch and waistband).
- All-in-one item of clothing can prevent gastrostomy removal (e.g. all-in-one swimsuit, full body suit).
- Specialist gloves (e.g. Posey Mitts).
- Nasogastric tubes may be maintained in situ by other methods but specialist advice will be required.
Repeated removal of a nasogastric tube may result in the need to insert a gastrostomy or jejunostomy tube. If tube feeding is anticipated to be required in the longer term it would be appropriate to consider a gastrostomy or jejunostomy tube at an early stage. This will help ensure safe administration of enteral feed resulting in nutritional and hydration requirements being met satisfactorily.
 Specialist advice and assessment should be sought if the patient makes repeated attempts to remove an enteral tube in order to decide if this method of feeding is essential. Such decisions are should be made by the responsible physician in liaison with the Speech and Language Therapist, Dietitian, nursing staff, family and any other relevant parties.
Specialist advice and assessment should be sought if the patient makes repeated attempts to remove an enteral tube in order to decide if this method of feeding is essential. Such decisions are should be made by the responsible physician in liaison with the Speech and Language Therapist, Dietitian, nursing staff, family and any other relevant parties.
Indications for Enteral Nutrition
Enteral Feeding Regimens