 There are three main types of intracranial haematoma which may occur following
There are three main types of intracranial haematoma which may occur following
traumatic brain injury:
- Extradural (or Epidural) haematoma
- Subdural haematoma
- Intracerebral haematoma/haemorrhage
Extradural Haematoma
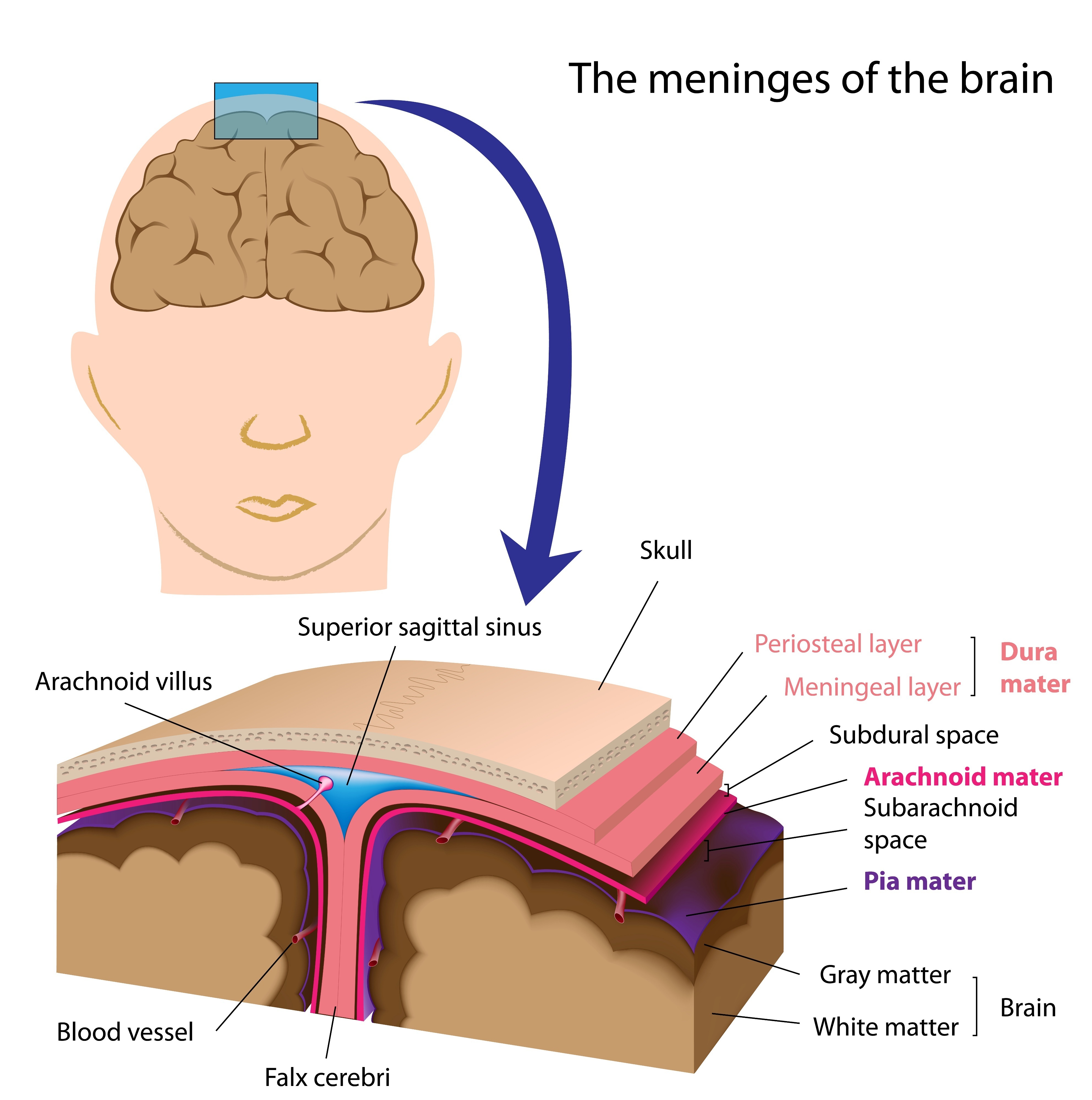
This describes a haematoma lying between the skull bone and the dura mater. It is called extradural as it lies outside the dura. It usually results from a skull fracture tearing arteries but can be due to damage to venous sinuses (channels) within the skull.
An extradural haematoma can take a few hours to accumulate so the patient may appear normal for a period of time following head injury (referred to as the ‘lucid interval’) before deteriorating and developing neurological symptoms. Close monitoring and CT brain scanning is essential as an extradural haematoma is a neurosurgical emergency.
Subdural Haematoma
The impact of an injury can rupture bridging veins which run through the dura mater. Blood accumulates between the dura and arachnoid maters i.e. below the dura mater resulting in a subdural haematoma. This is more common in older people as the brain shrinks with age making more room for movement within the skull.
A subdural haematoma may develop shortly after injury (acute subdural), one to two weeks after injury (subacute subdural) or more than two weeks later (chronic subdural).
Intracerebral Haematoma/Haemorrhage
This refers to an accumulation of blood within the substance of the brain (cerebrum) itself. It is not uncommon to have a combination of subdural and intracerebral haematomas.
In addition to the above haematomas, trauma can cause bleeding into the space between the arachnoid and pia maters resulting in traumatic subarachnoid haemorrhage.
Please note that intracranial haemorrhage may also be vascular in origin e.g. haemorrhagic stroke.